Introduction: Why Leukocyte Content Matters in PRP
Understanding leukocyte-poor PRP — and how it differs from leukocyte-rich PRP — is one of the most clinically useful distinctions a practice can make when choosing a preparation system. While many clinicians focus on platelet yield and preparation time, the white blood cell profile of a PRP preparation varies widely between systems. That variation matters for how you read the research and talk with colleagues.
This post explains what leukocyte-poor PRP means, how it compares to leukocyte-rich PRP, and why knowing your system’s exact cellular profile is worth the effort.
For a foundational overview of PRP preparation, see: What Is PRP?
What Is Leukocyte Content in PRP?
Whole blood contains red blood cells, platelets, plasma, and white blood cells — also called leukocytes. When a centrifuge spins the blood, those components separate into layers based on density.
The leukocyte layer, often called the buffy coat, sits between the red blood cell layer below and the plasma layer above. Specifically, it contains several white blood cell types:
- Neutrophils — the most abundant white blood cells in circulation
- Monocytes — precursors to macrophages involved in tissue remodeling
- Lymphocytes — part of the adaptive immune response
Depending on the centrifuge protocol and tube design, varying amounts of these cells end up in the final PRP preparation. The system then produces either leukocyte-rich or leukocyte-poor PRP as a result.
Leukocyte-Rich PRP vs. Leukocyte-Poor PRP: Key Differences
These two preparation types are not interchangeable. In fact, the distinction comes down to what the system retains — or removes — during centrifugation. Each approach produces a meaningfully different cellular profile.
| Characteristic | Leukocyte-Rich PRP (LR-PRP) | Leukocyte-Poor PRP (LP-PRP) |
|---|---|---|
| Neutrophil content | Elevated — buffy coat retained | Reduced — buffy coat excluded |
| Monocyte content | Variable | Can be selectively retained |
| Preparation approach | Typically includes buffy coat layer | Excludes or minimizes buffy coat |
| Inflammatory response profile | More pro-inflammatory | Lower inflammatory response |
| Common applications studied | Some tendon applications | Intra-articular, facial, scalp |
| Research landscape | Mixed findings across applications | Growing evidence base, particularly in knee OA |
Table for educational reference only. Clinical application decisions remain with the treating provider.
Why Neutrophil Reduction Defines Leukocyte-Poor PRP
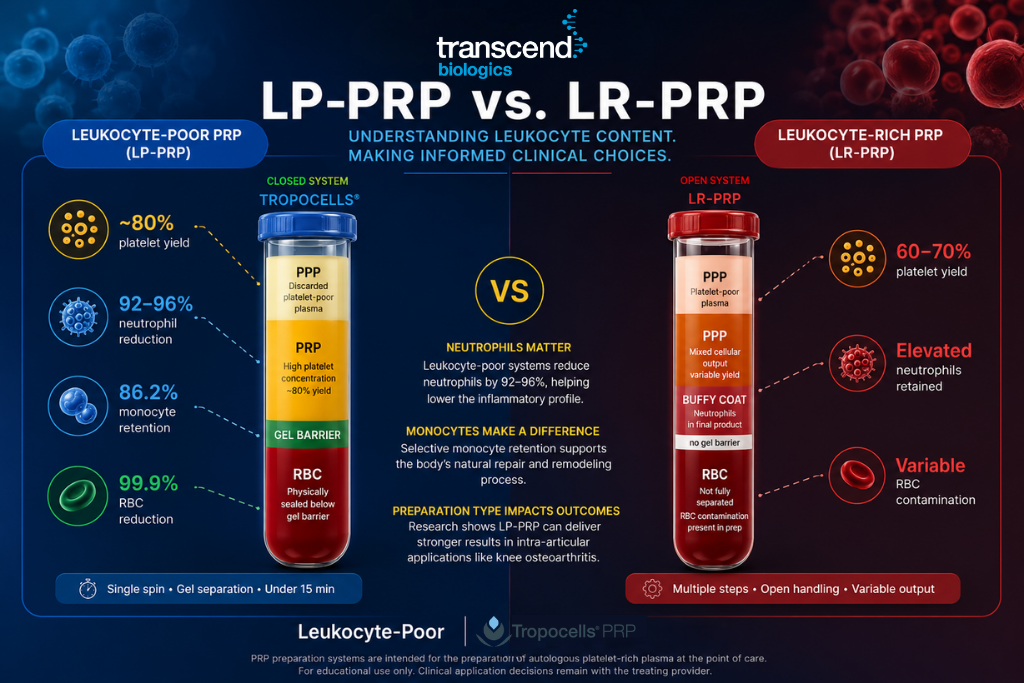
Neutrophils are the most abundant leukocyte in circulation, and they concentrate in the buffy coat layer. In a leukocyte-poor PRP system, the separation method actively excludes this layer — cutting neutrophil content by 92–96% in the final preparation. In a leukocyte-rich system, by contrast, the buffy coat stays in, and neutrophil levels in the product can rise well above baseline whole-blood levels.
Neutrophils play an important role in the body’s acute inflammatory response. However, their relationship to tissue repair in PRP applications is more complex. A 2014 study in the American Journal of Sports Medicine by Dragoo et al. compared LR-PRP and LP-PRP in tendon models. The study found that LR-PRP produced a more intense inflammatory response, while LP-PRP showed a different cellular profile.1
Similarly, a 2020 review in the British Journal of Sports Medicine (Kia et al.) analyzed 152 PRP studies and found that outcomes varied based on leukocyte content. The authors concluded that preparation type should be a standard reported variable in clinical research.2
For your practice, this means the PRP your system produces may differ from the PRP in the studies you read. Therefore, knowing your system’s actual leukocyte output is the first step in making sense of the literature.
The Monocyte Variable in Leukocyte-Poor PRP Most Practices Overlook
While neutrophils get most of the attention in LP vs. LR discussions, monocytes deserve a closer look. Monocytes are the parent cells of macrophages — the cells that drive tissue remodeling and the shift from the inflammatory phase to the repair phase of healing.
A 2019 paper in Frontiers in Immunology (Orecchioni et al.) showed that monocyte-derived macrophages play a key role in early-stage tissue repair. Specifically, their presence shapes the biological setting that follows injury or treatment.3
In practice, monocyte retention varies widely depending on the separation method. Some systems achieve strong neutrophil reduction by cutting the buffy coat entirely — which also removes most monocytes as a side effect. However, systems that use a physical separator, such as a gel barrier, can reduce RBCs and neutrophils while still keeping the monocyte fraction intact.
Furthermore, few vendors report monocyte retention as a standard metric. As a result, it is worth asking your vendor directly what the monocyte profile of your current preparation looks like.
What the Research Shows: LP-PRP in Intra-Articular Applications
Clinicians increasingly recognize preparation type as a critical variable when reading PRP research. A 2022 review and meta-analysis in Nature Reviews Rheumatology (Hohmann et al.) examined 18 randomized trials of PRP in knee osteoarthritis and found:
- PRP showed clear improvement over placebo in pain and function at 6 and 12 months
- LP-PRP showed stronger results than LR-PRP in intra-articular use
- The authors called for standard preparation reporting in future trials4
A 2021 meta-analysis in The American Journal of Sports Medicine (Belk et al.) found similar results — with PRP outperforming hyaluronic acid and placebo at 6 and 12 months in knee osteoarthritis, and preparation type emerging as a key variable in outcomes.5
These findings do not establish that LP-PRP treats any condition. Instead, they show that in the intra-articular literature, leukocyte-poor preparations produce a different response pattern than leukocyte-rich ones. Knowing which type your system produces is therefore essential for reading this research accurately.
How to Determine Your Current System’s Leukocyte Profile
Most PRP vendors can provide data that describes the leukocyte content of their system’s output. When you evaluate your current system — or compare alternatives — ask for the following:
- Neutrophil reduction percentage — how much of the neutrophil content the system removes relative to baseline whole blood
- Monocyte retention percentage — what fraction of monocytes the system keeps in the final preparation
- RBC reduction percentage — how much red blood cell contamination remains in the final product
- Platelet yield — the percentage of available platelets the system captures from the draw
- Preparation classification — whether the system produces LR-PRP or LP-PRP, and the basis for that classification
If your vendor cannot provide these figures, that gap is useful information in itself. You should expect validated preparation data from any commercial PRP system in clinical use.
For more on what to look for when evaluating PRP systems: PRP Preparation Systems
Tropocells: A Leukocyte-Poor PRP System With a Published Cellular Profile
Tropocells PRP is a leukocyte-poor PRP system that uses a patented gel separation mechanism. During centrifugation, the gel moves to form a physical barrier between the red blood cell layer and the platelet-rich plasma layer. That barrier separates the final preparation from RBC contamination without requiring manual aspiration technique.
The Tropocells preparation profile, based on validated system data:
- Up to 99.9% red blood cell reduction via gel barrier
- 92–96% neutrophil reduction in the final preparation
- >86.2% monocyte retention
- ~80% platelet yield from the original draw volume
- Up to 5 billion platelets from a 22 mL draw; up to 10 billion from a 40 mL draw
In short, this profile places Tropocells in the leukocyte-poor category. It achieves strong neutrophil reduction while keeping the monocyte fraction intact — through system design, not operator skill.
The treating provider determines clinical outcomes. These figures are preparation characteristics only.
Learn more about the Tropocells system: Tropocells PRP System
Reading PRP Research With Preparation Type in Mind
One of the most practical benefits of understanding LP vs. LR PRP is the ability to read clinical studies more accurately. PRP is not a single standard product — it is a category. Consequently, studies that use different preparation types can reach different results for legitimate reasons.
When you review a PRP study, it is worth asking:
- Does the study name the preparation type (LP-PRP or LR-PRP)?
- What system did researchers use, and do they report the cellular profile?
- Does that preparation type match what your system produces?
- Does the application in the study match your intended clinical use?
Two well-designed studies can reach opposite conclusions about PRP outcomes — not because one is wrong, but because they studied preparations with different leukocyte profiles. That is precisely why researchers have called for standard cellular composition reporting in PRP trials.
Conclusion: Why Leukocyte-Poor PRP Classification Matters
Leukocyte content is one of the most meaningful variables in PRP preparation — and one of the least consistently reported across commercial systems. Knowing whether your system produces leukocyte-poor PRP or leukocyte-rich PRP, and understanding the specific neutrophil and monocyte profile that follows, helps your practice read the literature accurately and talk about preparation with confidence.
To summarize:
- LR-PRP retains more leukocytes, including elevated neutrophils; LP-PRP reduces them
- Research suggests LP-PRP may produce a different response profile, notably in intra-articular use
- Monocyte retention is a separate and often missed variable in LP vs. LR comparisons
- Knowing your system’s cellular profile is essential for accurate literature review
- You should be able to get validated preparation data — neutrophil reduction, monocyte retention, and RBC reduction — from any commercial PRP vendor
For practices that evaluate their current PRP system or consider adding PRP, a focused conversation on cellular profile data is a practical first step.
Compare Your Current PRP System
Schedule a 10-minute call with the Tropocells team to review your current system’s cellular profile data and compare it against Tropocells’ preparation specs.
References
- Dragoo JL, et al. Comparison of the acute inflammatory response of two commercial platelet-rich plasma systems in healthy rabbit tendons. Am J Sports Med. 2012;40(6):1274–1281. doi:10.1177/0363546512442334
- Kia C, et al. Leukocyte-rich versus leukocyte-poor platelet-rich plasma: a systematic review of clinical outcomes in orthopaedic surgery. Br J Sports Med. 2020. doi:10.1136/bjsports-2019-101473
- Orecchioni M, et al. Macrophage polarization: different gene signatures in M1(LPS+) vs. classically and alternatively activated macrophages. Front Immunol. 2019. doi:10.3389/fimmu.2019.01084
- Hohmann E, et al. Platelet-rich plasma in the treatment of knee osteoarthritis: a systematic review and meta-analysis. Nat Rev Rheumatol. 2022. doi:10.1038/s41584-021-00703-5
- Belk JW, et al. Platelet-rich plasma versus hyaluronic acid for knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med. 2021. doi:10.1177/03635465211001321
Regulatory Notice: Tropocells PRP preparation systems serve the preparation of autologous platelet-rich plasma at the point of care. The treating provider determines all clinical applications and outcomes. This content serves educational purposes for licensed healthcare professionals. No clinical outcomes are claimed.
Additional resources: FDA Medical Devices | PubMed